
The Hearing Side of Usher Syndrome
I thought this one would be easy to write. It wasn't.
by Mark Hubers
I didn’t jump when a cop car hit its horn right behind me.
I was about three, just a happy kid who didn’t know there was a hearing world yet. That’s how my parents found out. Hearing aids ever since.
Tom V.A., a member of our community, calls hearing “the forgotten plain Jane of Usher syndrome.” He’s right. For those new to Usher syndrome, it takes both your hearing and your vision. Most of us are also going blind. My other essays cover the vision side. This one is about the ears.
We talk about the eyes. We talk about tunnel vision, night blindness, the shrinking world. But for most of us, the hearing loss came first. It was there from day one. Everyone else focuses on the eyes. We never stopped thinking about the ears. It’s always there. Always a struggle in some way.
This essay is about what’s going on inside your ear, what’s going wrong, and what it feels like to live it. I worked with sound processing long ago, so I’ll try to explain it the way I understand it.
So let’s start with something basic. Sound and noise aren’t the same thing.
Sound is what you’re trying to hear. Noise is everything else. A hearing person’s brain sorts them apart without thinking about it. Ours can’t. Everything comes in at once and competes for the same space.
If you’re hard of hearing, noise feeds on the little you have. Every fan, every TV, every voice in the background eats into the words you’re trying to catch. The hearing world tunes it out. We can’t. It stacks up until the words we need are buried.
Not just restaurants. Anywhere outside your own home. Even at home, someone has a TV on and thinks you should hear fine. You don’t. But you let a lot of it slide because you have to pick your battles.
If you’re profoundly deaf, sound is everything you’re not getting. All of it. The whole room. Not just the conversation you’re missing. The music, the laughter, the door that just closed behind you, the phone that slipped out of your pocket or off your lap and you didn’t hear it hit the floor. Most people never stop to think about what that means.
Two different kinds of loss. Both invisible. Both exhausting in their own way. And both living in the same hearing world.
I’ll say something to my deaf and hard of hearing friends that not everyone wants to hear. And if you’re hearing, stay with me. Your part is coming.
This is a two-way street. We have to accept that.
We can’t expect everyone around us to learn sign language, the same way we can’t expect everyone to learn every language on earth. You’d leave someone out no matter what.
But the people close to you, your family, your friends, the ones who matter, they should try. And to those people: face me when you talk. Get my attention first. Turn the TV down.
That’s the other side of the two-way street. We meet the world halfway, and the people who love us meet us the other half.
Learn when you need to be heard, and learn when to let it go. That’s hard to take. But that’s life.
That’s just how I see it. I don’t do this often in my essays, and I’ll try not to make a habit of it. But sometimes you have to say what you actually think.
If someone in your life has hearing loss, this is what they’re not telling you. Not because they don’t want to. Because it’s hard to put into words. That’s what I’m trying to do here.
HOW HEARING ACTUALLY WORKS
Your inner ear has a tiny spiral about the size of a pea (the cochlea). It’s filled with fluid that carries the sound in. Inside it are thousands of hair cells, and those hair cells are how you hear.
Think of them as tiny grass blades standing in rows, nice and straight when there’s no sound. Short ones, medium ones, tall ones, lined up like a staircase.
When sound enters the cochlea, it creates waves in the fluid. The waves bend the shorter hairs into the taller ones, and that triggers a switch. That switch creates the electrical signal your brain hears. There’s a lot more going on at that level (stereocilia mechanotransduction), but that’s the basic idea.
That signal travels through the hearing nerve (auditory nerve) to your brain, and your brain turns it into “I heard the word ‘hello.’”
That part is simple. Short hairs bend into the tall ones and a switch triggers. Easy enough. But my engineering brain won’t leave it alone. The tall one is bigger, so shouldn’t the waves move THAT one more? Why does the short one do the work? It doesn’t matter for this essay, but I wanted you to see how my brain works. I’m always pulling things apart, even the basic stuff. That’s just how I think.
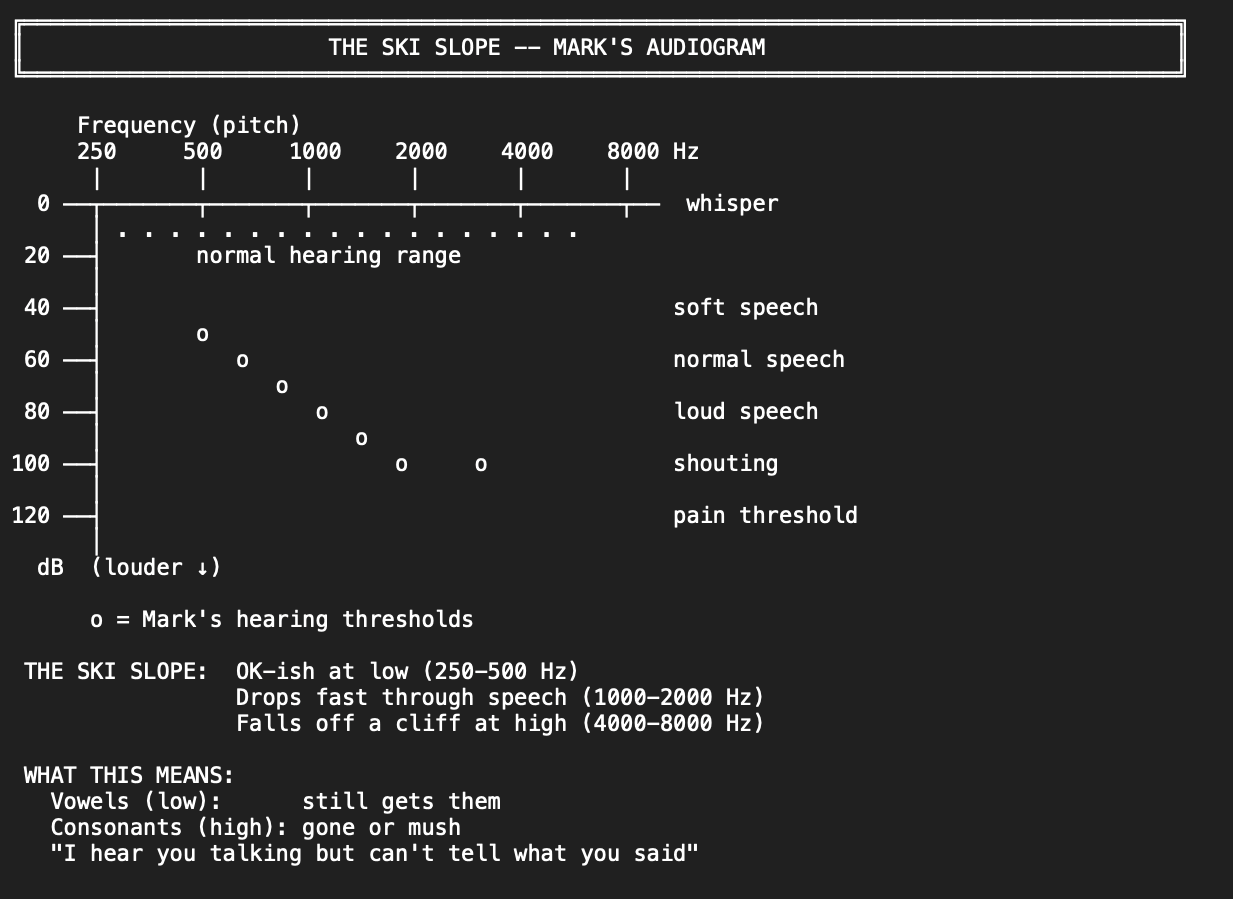
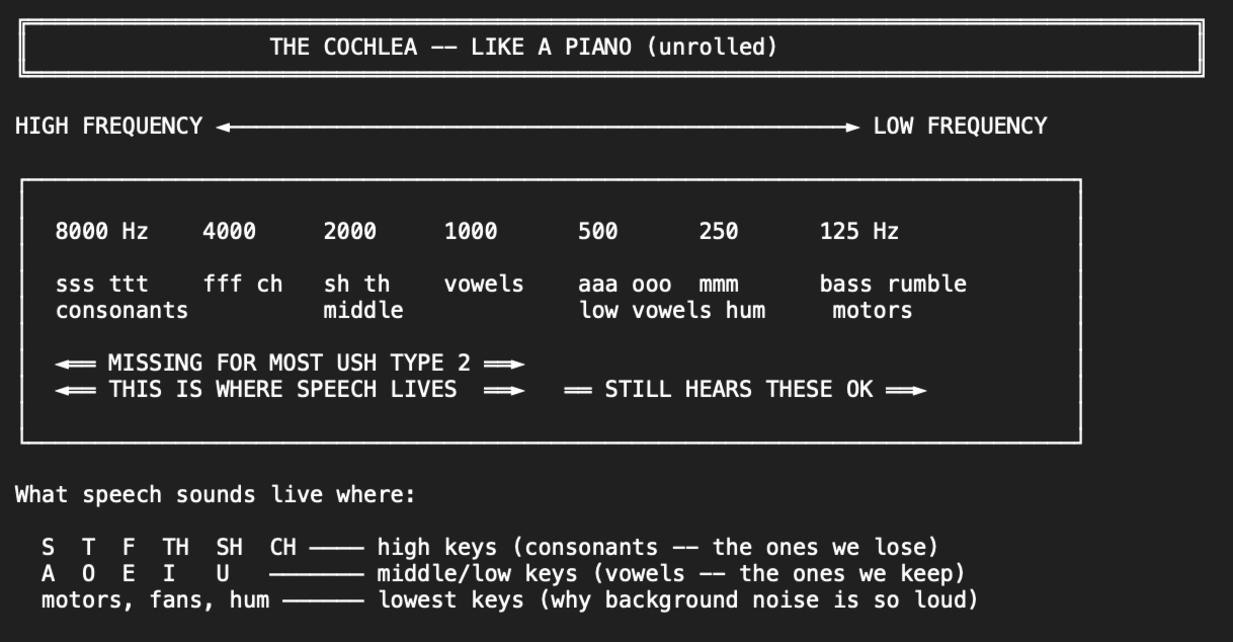
The cochlea maps sound by location. Think of it like a piano. High notes on one end, low notes on the other. Your cochlea works the same way. Every sound you hear uses some combination of those keys.
That's the menu. Five fundamentally different approaches, each with different trade-offs. And the first thing you should notice is that most of them don't require knowing your gene at all.
The hair cells are connected to each other by tiny protein threads. The ones at the tips are called tip links. The ones at the base are called ankle links. When those connections are broken, the keys stop working.
Each Usher type has different connections broken. Some are missing almost all their keys from birth. Some were born without the high keys and never had them. Some start with most keys working and lose them over time.
WHAT IT’S ACTUALLY LIKE
This is how it works for me. If you still have some good hearing, count yourself lucky, but a lot of this will still feel familiar.
For those who are profoundly deaf and losing vision, it’s different and in some ways harder. Some are reading signs by placing their hands on the signer’s hands to feel the shapes being made (tactile sign language), because they can’t see the hands or hear the voice. Some of us may end up there one day. I hope I don’t, but I can’t promise that. What I can say is there’s more hope now than ever. Gene editing, pills that slow the damage, treatments that stabilize what’s left. The science is moving. We all have our own version of this fight.
When someone says a word, that word needs certain keys to sound right.
If the word uses keys you don’t have, you don’t hear silence where that sound should be. The sounds around it bleed into that space. The tone shifts.
What reaches your brain is a distorted version of the word, not a word with a hole in it. Your brain takes that mess and pattern-matches it to the closest word it knows. Sometimes it’s right. Sometimes you hear a completely different word that sounded close enough.
Say someone says “think.” The TH is on a high key I don’t have. But I don’t hear “ink.” I hear something that sounds like it could be “think” or “fink” or “sink” because the sounds next to it color what I get. My brain picks one. If the conversation is about ideas, it picks “think.” If we’re talking about a kitchen, maybe it picks “sink.” Context does the work my ears can’t.
And some sounds just disappear entirely. The S at the end of a word has nothing after it to bleed into. It’s just gone. So “cat” and “cats” sound the same to me. One or many? I have to figure that out from the rest of the sentence, if the sentence was long enough to give me a clue.
The harder ones are words that start with a sound you don’t hear. You’re already behind before the word even gets going. By the time you catch the middle, you missed the opening and your brain is guessing from half a word.
Here’s what a sentence sounds like to me versus you.
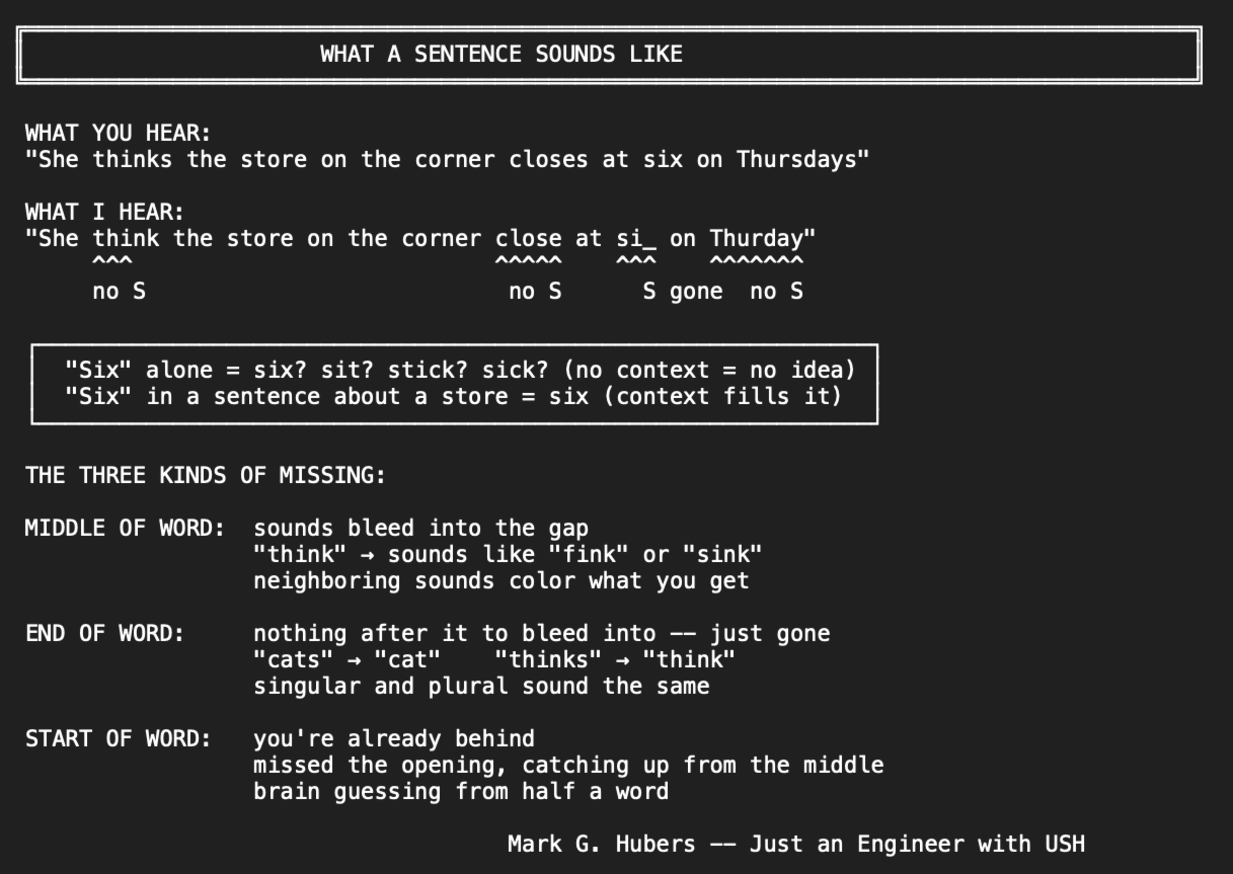
Say someone says: “She thinks the store on the corner closes at six on Thursdays, so we should probably leave before five thirty if we want to make it.” That’s a long sentence. I hear: “She think the store on the corner close at si on Thurday, so we should probably leave before five thirty if we want to make it.” The S’s are gone. Thinks becomes think. Closes becomes close. Six could sound like sit. Thursdays becomes Thurday. But I got most of it because there’s enough flow. Enough words around the missing ones to fill in what I didn’t hear. My brain adds back the S’s because it knows how sentences work.
Now say someone just says: “Six.” By itself. Did they say six? Sit? Stick? Sick? I have no idea. Same word, but with nothing around it, I can’t tell. Or “She thinks so.” Three words. Not enough to build on. Think becomes thi–, she becomes ee, so is fine. But I’m guessing at two out of three words.
The longer someone talks about the same thing, the better I follow. The shorter the sentence, the harder it is. One or two words by themselves? I might not know any of them. But even a long sentence can fall apart if I miss too many words in a row. Enough gaps and the whole thing collapses no matter how long it is.
And here’s something nobody talks about.
My brain doesn’t just process forward. It goes back. Say I hear a word wrong early in a sentence. I keep listening. Five or ten words later, new context comes in and my brain goes back and replaces the wrong word with the right one.
I didn’t hear it better. My brain figured out what it had to be from what came after. Sometimes I can feel it happen. A word I thought I heard gets quietly replaced with the right one.
I’m not just listening. I’m running a prediction engine forward and a correction engine backward at the same time.
And here’s what that costs: while my brain is going back to fix the words it got wrong, I’m missing the new ones coming in. For a moment, I’m offline. Rebuilding the past and losing the present at the same time. Then I come back and have to catch up on what I missed while I was fixing what I misheard.
If you want to know what this feels like, think about learning a new language. Remember trying to follow someone speaking French or Spanish? You catch a few words, guess the rest, your brain goes back and corrects, and while it’s correcting they’ve moved on. Short sentences are harder than long ones. You’re exhausted after thirty minutes. That’s what hearing loss is. Except it’s in your own language. Not because we don’t know it. Because we can’t hear every word right. And it’s every conversation. All day. For life.
And that’s the hardest part of all. Following a conversation is like building a puzzle without the picture on the box. You start catching pieces, matching them to context, using lips and tone and what you know about the topic. After a minute or two, you’re keeping up. You’re in it.
Then someone changes the subject. That’s not rude, that’s just how people talk. One thing leads to another. Everyone wanders, the same way you wander the internet or scroll through your phone.
But for us, every topic change is a crash back to zero. All that context you built is gone. You’re starting over with no picture, no pieces, trying to figure out what they’re even talking about now. That happens over and over, all day.
So how can you help?
Watch for it. If you see us go quiet or our face changes, we probably just lost the thread. Don’t keep going. Stop. Say “we just switched to talking about…” and give us the new topic. That one sentence puts us back in the game.
Ask us if we’re following. And if we ask you to repeat, please just repeat it. Don’t sigh. Don’t get frustrated. Don’t hit us with “I SAID…” We know you said it. We’re not asking to annoy you. We’re asking because we want to hear you.
And don’t say “never mind” or “I’ll tell you later.” There is NEVER a later. That moment passes and it’s gone. And every time you say it, it hurts. It was important enough to say once. Say it again. Without the sigh. Without the look on your face that tells us we’re a burden for asking.
And I haven’t even told you the worst part yet. Most of us with Usher syndrome are also losing our vision. The lip reading I depend on? I can’t always see your lips. They move too fast for eyes that can’t track motion anymore.
And just about everywhere people hang out is dark. Bars, restaurants, movie theaters, concerts. The places the hearing world goes to be social are the exact places where I can’t see your face AND can’t hear your voice. Both systems failing at the same time, in the same room.
I know that’s hard to read. It’s harder to live it.
OK. Back to the essay. On top of everything I just described, every device in the chain makes it worse. Phone speaker to hearing aid, TV across the room to hearing aid, each layer adds noise to an already bad signal. A bad signal amplified is a worse signal, not a better one. That’s why Bluetooth was a game changer for us. Sound goes straight from the phone or TV to the hearing aid or cochlear implant without passing through the air. One less layer of mess.
And if you went to speech therapy, you know the hardest part. They ask you to make sounds with your mouth that you have never heard. Think about that for a second. That’s like someone describing what a pangolin sounds like and then asking you to do it. You’ve never heard one. Now make the sound. That’s speech therapy for us.
THE THREE TYPES
Not all Usher syndrome is the same.
The type you have determines which keys are missing, how many you start with, and whether you keep losing more. What I’m about to describe is the basic picture of each type, roughly what things look like by the late teens as a reference point. Type 1 and Type 3 can vary a lot, and the lines between the types aren’t as clean as the textbooks say. I’ll get deeper into each type in a later essay. For now, this is the overview.
Type 1: The switches are broken.
The tip link proteins (the connections at the top of the hair cells) are broken or never formed. The hairs splay outward in all directions like fingers spreading. Some switches stuck on, some stuck off. No coordinated signal. Profound deaf from birth.
Some people with Type 1 do have a little hearing early on, but it fades fast because the protein that maintains the switches is also the one that keeps them working day to day.
Hearing aids can’t fix this. No amount of louder helps when the hairs are a mess. That’s why most people with Type 1 get cochlear implants (CI). A CI bypasses the hairs entirely and sends electrical pulses directly to the hearing nerve, doing what the hairs would have done.
Type 2: The foundation is weak.
The ankle link proteins (connections at the base) are malformed. The switches at the top work fine. But the whole structure is leaning because the base is soft. Like a light switch mounted on a wobbly wall. You can still flip it but sometimes it catches, sometimes it doesn’t. The signal gets through, but it’s messy.
Hearing aids help by pushing the sound louder to overcome the lean. It takes more energy to trigger a switch when the thing it’s mounted on isn’t stable. That’s why we need powerful hearing aids. And it stays about the same. The foundation doesn’t keep getting weaker. Your hearing loss is severe, but it’s stable.
Type 3: Everything fails over time.
Everything works at first. The hair cells grow normally, the connections form, the signals fire. But over time, the protein that sustains the cells (clarin-1) can’t keep up. The hair cells degrade and die. You start with most of your hearing and lose it over time. This is the rarest type, and the hardest to plan around because nobody knows how fast it will go.
Types 1 and 2 have broken parts from the start. Type 3 has a broken maintenance system. That’s the difference.
What tends to help, and when:
Hearing is a spectrum, just like vision. No two people hear exactly the same even with the same type. What I’m about to say is the general picture, not a rule.
Type 1 usually needs cochlear implants early.
The earlier the better for the brain to learn what to do with the signal. Hearing aids alone can’t overcome the damage.
Type 2 usually does well with hearing aids for most of life.
Powerful ones. The aids push louder to overcome the leaning hair cells. At some point, usually later in life, the hearing aid ceiling gets close and the CI conversation starts.
Type 3 is the hardest to plan for.
Hearing aids work at first, then need to keep getting stronger as the hearing drops. The timing of when to switch to CI depends on how fast it’s going, and nobody can predict that.
All of this should be done with an audiologist, not a hearing aid dispenser. I’m not putting dispensers down. Places like Costco are great for people with age-related hearing loss who had good hearing most of their life. But for USH, you need a doctor who understands the kind of damage we’re dealing with. It’s a different problem.
And while I’m on that subject, people always ask why our hearing aids cost 3 to 5 times more. It’s not just “louder.” Think of it this way. Go buy a nice cheap Bluetooth speaker. Sounds great in your living room. Now take that same speaker outside to a loud party, turn it to max, and try to hear someone talking over a crowd. It sounds terrible. It distorts. It can’t handle it. It wasn’t built for that. Now look at a professional speaker system that costs ten times more that handles a party no problem. Clear at high volume, cuts through noise, doesn’t distort. That’s the difference between a basic hearing aid and what we need. Our aids have to run at extreme power without distorting, suppress feedback, separate speech from noise, all in something the size of a fingertip. That’s deep engineering, and it costs what it costs.
And here’s what makes it worse. Insurance and most workplace plans still lump us in with age-related hearing loss. They cover the cheap speaker when we need the professional system. The hearing aids we need cost thousands, not hundreds. Most of us with USH don’t have high-paying jobs. Some don’t have jobs at all. And hearing aids are just one cost. Add to that the retina specialists, the cornea doctors, the scleral lenses, the low vision evaluations. I’ve worked full time my entire adult life. I’m in meetings every day. I hear and talk and contribute because of these hearing aids. My insurance still doesn’t cover them. Apparently they’re “nice to have.” Without them I can’t do the job. With them, I pay for them myself. Either way, we lose. USH is expensive to live with, and the system hasn’t caught up to what it actually takes. If you’re outside the US, I hope your country does a better job covering this. Here in the states, there’s no federal law that requires insurance to cover hearing aids.
One thing to know about cochlear implants: it’s not something you can undo. The surgery destroys most of the remaining hair cells in that ear. Once you go CI, you can’t go back to hearing aids in that ear. That’s why the timing matters so much. A hearing aid amplifies what you have. A CI replaces it entirely with electrical pulses. Both are doing the same job – getting sound to the brain – but through completely different paths.
For all three types, the earlier you act, the better the brain adapts. The brain learns to use whatever signal it gets. Wait too long and it gets harder.
Each type also has subtypes based on which specific gene is involved. Type 1 alone has five different genes (USH1B, 1C, 1D, 1F, 1G). Type 2 has three. Type 3 has one. The gene matters because it determines which treatments might work for you in the future. That’s a whole separate topic and I’ll get into it in a later essay about knowing your gene.
If you want to know a little more about each type, I have some extra notes at the end of this essay. And for how the types cross over and what the genes actually do, that’ll be a later essay.
WHY IT SEEMS TO GET WORSE
If Type 2 is stable, why does it feel like my hearing is getting worse in my 50s?
Melinda is Type 2, in her 50s, and she asked me: “Am I imagining it, or is my hearing getting worse?” My friend Bart isn’t even USH. He’s just hard of hearing, same loss as me, same aids for 30 years. He says it’s harder now too. We’re both 58.
But our hearing tests (audiograms) haven’t really changed that much. What changed is us. Our brains are slower. The world got noisier. And the keys we still have are tired. They’ve been carrying the whole piano for over fifty years.
This matters because it changes what you do about it.
If the gene is progressing, there’s not much to try right now. If it’s the brain aging, there are things that help. Better hearing aids. Auditory training. Knowing when it’s time to talk about a cochlear implant. The answer to “is my hearing getting worse?” might be: your USH2 hasn’t changed, but your brain’s ability to work with that messy signal is declining with age. That’s a different problem with different solutions.
Nobody tracks any of this. Everyone shares their experience. Nobody shares their variables. Age at loss. Age at testing. What they heard before. What they hear after. How long between. One ear or both. What brand of aid, what settings, what environment. Without those numbers, community advice is just anecdotes arguing with each other. The data gap for hearing in Usher syndrome is the same gap I found in the vision research: everyone has pieces of the answer, nobody is putting them together.
Hearing loss is the invisible tax. You can see that someone uses a cane. You can’t see that their brain is burning through its daily budget just to follow a conversation at lunch.
THE WINDOW IS SMALL
When you have both conditions, hearing isn’t a preference. It’s your remaining lifeline.
As RP takes peripheral vision, your brain leans harder on sound for spatial awareness. Where is the door? Is someone behind me? Did I leave the water running? Normal peripheral vision handles most of that without you thinking about it. When it’s gone, sound picks up the slack. And when the sound is already damaged by hearing loss, the slack isn’t much.
I have about 30-35 decibels of headroom. My hearing loss sits around 97-100 dB (that’s severe-to-profound). My hearing aids, running UltraPower receivers, max out around 132 dB. That’s the absolute ceiling of what hearing aid technology can deliver. Normal hearing uses about 100 dB of range. I work with a third of that.
Put my hearing aid on a normal-hearing person and you’d cause immediate permanent damage. The aid puts out over 130 dB. That’s a jackhammer at one meter. OSHA won’t let workers near 115 dB for more than 15 minutes. But for someone with my loss, 130 dB is Tuesday.
The window between “can’t hear it” and “hearing aid can’t go louder” is small. And it’s all I’ve got. When that window closes, the next step is a cochlear implant. I’m not there yet. But I’m at the edge.
THE FORGOTTEN SENSE
People ask about my vision. They don’t ask about my hearing.
Maybe it’s because hearing loss doesn’t look dramatic. There’s no cane, no dark glasses, no white-knuckle moment at the crosswalk. I’m in a meeting, I’m nodding, I seem fine. What they don’t see is the engine running at full speed underneath, trying to build whole words out of missing keys, guessing what you said, hoping I guessed right, all while also tracking what my eyes can’t.
Hearing loss in Usher syndrome isn’t just “turn it up louder.” Louder doesn’t bring back keys that were never there. It’s an invisible tax that compounds with the invisible tax of losing vision. Two systems failing independently but experienced together.
Tom was right. Hearing is the forgotten plain Jane. But for those of us living with both, it’s the sense we can’t afford to forget.
To my deaf and hard of hearing friends without USH, a lot of what I wrote here is your life too. I’m working on something just for you.
OK. I always tell myself I’m going to keep these essays short.
I always fail. Sorry about that. If you’re done, you can stop here. If you want to know a little more about what’s different for Type 1 and Type 3, I have a bit more below. It’s not the full story on each type. I’m still learning when to cut my losses and stop writing.
A Bit More on Type 1
Most people with Type 1 are profoundly deaf from birth or very close to it. But it’s not always zero from day one. Some have a little hearing early on that fades fast. The protein that builds the tip links (the switches) is the same protein that maintains them. So even if they form partially, they break down without ongoing maintenance.
Cochlear implants are the main path for Type 1.
The earlier the better. Tom got his first CI in 2002. It took twelve years before voices and music clicked. His second CI in 2025 merged with the first in one hour. The brain already knew how. That’s the timing argument in one story. First time is slow. Second time is fast. And every year you wait makes the first time harder.
A Bit More on Type 2
Not much more to say.
That’s actually the point. Type 2 hearing stays about the same most of our lives. The essay you just read is mostly written from that perspective. The changes we feel in our 50s and beyond are more about aging than the gene. I covered that above.
A Bit More on Type 3
Type 3 is the hardest to live with in some ways because you don’t know what’s coming.
You start with good hearing. It works. Then it starts to go and nobody can tell you how fast. Some lose it over a decade. Some over decades. Some hold on longer than expected.
The hearing aids that worked last year might not work next year. The settings keep changing. The audiologist keeps adjusting. And you keep asking the question nobody can answer: when does this stop? For Type 1 and Type 2, the answer is simple. Type 1 starts deaf. Type 2 stays about the same. Type 3 is the one where you’re always watching, always wondering.